Susan L. Clubb, DVM
Rainforest Clinic for Birds and Exotics, Inc., Loxahatchee, FL, USA
OVERVIEW OF ISSUE
Proventricular Dilatation Disease (PDD) is a devastating disease for affected birds. It is also psychologically and financially devastating for their owner/caretaker. Recent finding of a novel Avian Bornavirus in birds affected with PDD has created new hope for accurate diagnostics to enhance management of affected birds and flocks.
OBJECTIVES OF THE PRESENTATION
- Present new research identifying possible etiologic agent.
- Review diagnostic procedures.
- Present management and treatment options.
KEY ETIOLOGIC AND PATHOPHYSIOLOGIC POINTS
A viral etiology has long been suspected for PDD and numerous viral agents have been found in birds affected with PDD, recently a strong association has been proposed with a novel virus, Avian Bornavirus. In analysis of 2 PDD case-control series collected independently in Florida and Israel, Avian Bornavirus was found by using a pan-viral microarray assay. Bornavirus was found in 5 of 8 (62.5%) birds affected with PDD and none of 8 controls. Ultra high throughput sequencing was utilized to recover the complete viral genome sequence. This virus was also found to have a high degree of sequence divergence from all prior known Bornavirus isolates. Subsequent PRC analysis of additional positive and negative samples revealed significant difference in ABV detection among PDD cases (71%, n=7) compared to controls (0%, n=4). Partial sequence analysis of a total of 16 isolates reveals at least 5 distinct ABV genetic subgroups.
Studies are proceeding at the time of writing in an attempt to prove if Avian Bornavirus does cause PDD. Additional cases and controls are being tested in order to detect additional strains of the virus which may be present in captive psittacine birds.
KEY CLINICAL DIAGNOSTIC POINTS
- Laboratory diagnostics should be available soon if Avian Bornavirus is proven to be the etiologic agent.
- At this time pathological evidence obtained by crop biopsy or necropsy is still needed to confirm the disease.
- Clinical signs, radiography, fluoroscopy and clinical pathology are all useful adjuncts to clinical exam for making a diagnosis.
KEY CLINICAL MANAGEMENT OBJECTIVES
The diagnosis of PDD in an avicultural collection can have devastating financial effects on aviculturists. Counseling as well as establishing a long-term management plan are important aspects of veterinary care. As diagnostic screening becomes available and positive birds can be identified, management will be much easier.
The social implications of a PDD diagnosis can also be devastating. Owners may be shunned from bird club functions or social interaction with other bird owners, or find it impossible to find a pet sitter. Counseling for owners needs to include the fact that PDD can be hard to diagnose, can take many forms and can have a very long incubation period. We have found visually healthy birds that were crop biopsy positive for PDD. We have also found cases with very subtle signs in which Avian Bornavirus has been detected by PCR of blood and cloacal swabs.
Waiting for the classic clinical signs such as wasting, vomiting or passing whole seeds will reveal only the tip of the iceberg. The bird owner should be encouraged to assess the disease status of his or her other birds, considering each bird individually. To be in denial and avoid checking other birds in the home is placing them at risk. In our experience, early diagnosis can enhance therapeutic outcome. Mates of birds that succumb to PDD should not be automatically euthanized. These birds may have natural immunity to the disease and may be the best future breeders for an avicultural community hard hit by PDD. In consultation with your client develop a treatment and control plan. Encourage your client to make the commitment not to bring more birds into the home, placing them at risk, or transfer exposed birds to others without disclosure.
Until causation is confirmed, histopathology of crop biopsy or tissues at necropsy is still the only definitive diagnosis of PDD. While crop biopsy has a high false negative rate, it is still a useful screening tool. Other helpful tests include radiographs, endoscopy and hematology and chemistry profiles. An exceptional test for live birds is fluoroscopy but this is rarely available to private practitioners. (Gregory, 2002, Boutette & Taylor, 2002)
As an infectious disease that causes inflammation of the nerves and affects the digestive system we must think about--preventing spread, reducing inflammation, aiding digestion and controlling secondary infections. And we must do this for a long time, probably a year or more.
KEY THERAPEUTIC POINTS
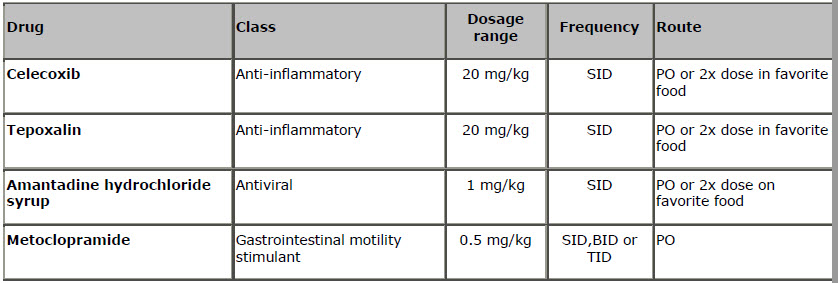
Initial reports of treatment using the anti-inflammatory drug Celecoxib presented the first real hope for birds affected with PDD. (Dalhausen et al, 2002) Nonsteroidal anti-inflammatory drugs ("NSAIDs") are a group of structurally diverse compounds used clinically for the successful treatment of a range of disorders that are associated with pain and/or inflammation. NSAIDs are known to inhibit the cyclooxygenase ("COX") enzymes, which catalyze the conversion of arachidonic acid to the various prostaglandins, and the drugs are believed to exert their analgesic and anti-inflammatory effects through inhibition of the COX enzymes. While the lymphoplasmacytic infiltrates in ganglia appear to be reversed as evidenced by repeated crop biopsies, this drug cannot be considered a preventative or a cure.
We dose Celecoxib at 20 mg/kg once daily if given directly orally. Compounding is not necessary as Celecoxib (in capsule form) dissolves well in water. We use one 200 mg capsule in 10 ml water and dose at 1 ml/kg BW. Fresh dilutions should be made as frequently as possible as we have observed treatment failures which we feel have been associated with mixing batches which were not used quickly. The length of time that Celecoxib is stable in water is unknown. Unless a bird is extremely tame, it will be stressed by daily oral dosing. We have had very good success in adding Celecoxib to the bird's food. We double the dose (40 mg/kg) when we give it in food since we expect them to lose half of it. We also give the medication on a small amount of food, preferably foods which will absorb the drug, so the chance of them eating it is improved. In most birds therapeutic response is gradual and many birds do not show much benefit for at least 2 weeks. Full recovery of a clinical case is slow and gradual.
We have also successfully used tepoxalin (Zubrin, Schering Plough) in a pilot study comparing the use of tepoxalin to Celecoxib. Tepoxalin is a combined COX-1 and COX-2 inhibitor as well as a LOX inhibitor (inhibits 5-Lipoxygenase pathway).
An important potential side effect of Celecoxib, and other COX 2 inhibitors in humans, is bleeding in the gastro-intestinal tract. (Clemett, 2000) An adult female Catalina hybrid macaw (Ara ararauna x Ara macao) that was crop biopsy positive for PDD, died within 7 days of initiation of Celecoxib therapy exhibiting an acute hemorrhagic event in the proventriculus on necropsy. We routinely monitor birds for development of melena, which could indicate proventricular or intestinal bleeding. In such cases, Celecoxib is discontinued immediately and the bird is evaluated, including a gram stain to detect Clostridium in the feces. A mature female hyacinth macaw (Anodorhynchus hyacinthinus) also seemed to develop hypersensitivity to the drug. This bird had inflammatory skin disease as diagnosed by paired skin biopsy. She developed severe pruritus locally on the sides of her face while being treated with Celecoxib, which subsided in severity when Celecoxib therapy was discontinued. Most NSAIDS are eliminated by renal clearance and should be used with caution in birds with renal disease. Nephrosis associated with NSAID use in birds is poorly documented. (Echols, 2004)(Echols, 2004)
Husbandry Considerations
If possible, keep the birds in roomy cages outside where sunlight and fresh air will help to dilute/inactivate the virus (if present). It will also enhance their general well being. Try to keep stress to a minimum.
In clinically affected birds diet should be easily digested since proventricular and ventricular function is affected and GI motility is reduced or delayed. Liquid diets are available commercially for birds that are severely affected. (http://birdcareco-shop.com/) Extruded diets (pellets) are good for birds during the long recovery phase since they are easier to digest than seeds. An extruded diet also works well because Celecoxib diluted in water is absorbed into the food.
Supplementing the diet with vegetables that are high in fiber might be beneficial to early cases by stimulating intestinal motility. Cruciferous vegetables are also beneficial sources of raffinose sugars (rich in oligofructosaccharides) which enhance viability of autochinous flora (Lactobacillus and Bifidobacterium), thereby inhibiting gram-negative bacteria andClostridium. (McDonald, 2003) In advanced cases however these foods may linger in the intestines and ferment. Periodic supplementation of probiotics is beneficial.
Birds with PDD often become anemic and hypo-proteinemic. (Boutette, 2004) The addition of powdered protein supplements such as egg or soy protein provides a readily utilizable source of protein. We utilize B complex vitamin supplementation to help correct anemia. We also supplement with Salmon oil, flax seed oil and safflower oil as sources of omega 3 and omega 6 fatty acids. My goal in fatty acid supplementation is 50-250 mg/kg body weight of Omega 3 fatty acids with an omega 3:omega 6 ratio of 1:2-1:6. When supplementing extruded diets I use a balance supplement of salmon oil and flax seed oil (high in omega 3 fatty acids) and safflower seed oil (high in Omega 6 fatty acids). If the bird is eating a primarily seed diet I supplement only with salmon oil and flax seed oil.
Birds with PDD often develop secondary bacterial and fungal infections, especially intestinal infections, because the intestinal motility is poorly coordinated and transit time is increased. These infections should be diagnosed and treated appropriately. In our experience, Clostridium infections are common in birds with PDD and can result in bulky, black, foul smelling feces and potentially death due to necrotizing enteritis. Vaccination for clostridium should be considered. I use a multi-valent bovine clostridium vaccine, administering 0.25 to 1 ml intramuscularly or subcutaneously. Initially two doses are given two weeks apart with an annual booster. (We have used a number of products but are currently using Vision 8, Intervet Inc, Millisboro, DE).
Gas formation and retention in the gastrointestinal tract is a common finding in birds affected with PDD and can cause discomfort. Gas may be evident radiographically but gas bubbles are also often present in the feces or vomitus. Surfactants provide some symptomatic relief. (Infant's Mylicon, Johnson & Johnson, Merck Consumer Pharmaceuticals). Many birds exhibiting gastrointestinal gas or vomiting respond clinically to combination drug therapy as if they haveHelicobacter although infection with Helicobacter has not been confirmed in them. We use Clarithromycin (Biaxin, Abbot Labs), Metronidazole and sucralfate (Carafate) (sucralfate, Axcan Scandipharm.)
If PDD affects the central nervous system, the prognosis is guarded. Affected birds show incoordination, tremors, and seizures.
We have found amantadine, an antiviral agent which also has anti-Parkinson's effects in humans, to be very helpful in management of cases exhibiting CNS signs. (Amantadine hydrochloride syrup, 50 mg/5 ml--HI-Tech Pharmacal Co, Inc, Amityville, NY, 11701). Amantadine was originally used for treatment of influenza (in humans) but was also found to be beneficial in treatment of Parkinson's disease, traumatic head injury, dementia, multiple sclerosis and cocaine withdrawal. It is a dopaminergic, nonadrenergic and serotonergic substance and serves as an anti-depressant. We have found the combination of Celecoxib and amantadine (1 ml/kg gm body weight orally SID, or 2 ml/kg in food daily) to be very beneficial in birds exhibiting CNS signs or birds with severe gastrointestinal dilation. Based on long term health monitoring and serial crop biopsies, we feel treatment must be prolonged in birds that are clinically affected-possibly up to a year or more.
We have found metoclopramide to be an important adjunct to management of severe cases. (0.5 mg/kg, q 12, PO, or IM) (Carpenter, 2005). We use it in cases with delayed intestinal transit time or intestinal stasis, initially administered by injection and later given orally as the intestinal tract regains motility. (Metoclopramide injection, 5 mg/ml, GensiaSicor, Irvine, CA and Metoclopramide Oral Solution, 5 mg/5 ml Morton Grove Pharmaceuticals, Inc, Morton Grove, IL 60053). An adverse reaction to metoclopramide has been reported in a macaw being treated for PDD. (Massey, 1993) Nutritional adjuncts to therapy that may be beneficial in cases with CNS signs include ginkgo biloba, Vitamin E, alpha lipoic acid, acetyl-L-carnitine and B complex vitamins.
Monitoring Progress of Therapy
Therapy can be monitored by periodic physical exam, monitoring body weight, repeated radiographs and evaluation to detect secondary infections. If monitoring by radiography the composition of the diet must be considered, especially if the bird was initially eating a primarily seed diet at the time of diagnosis and is later changed to an extruded diet. In my experience, birds eating a primarily formulated or extruded diets tend to have a relatively dilated gastrointestinal tract as evident by radiography that can complicate evaluation.
Birds affected with PDD often ingest foreign bodies, especially pieces of wood. These materials may then be passed in vomitus or feces. The bird may be ingesting these materials in an attempt to provide relief from intestinal discomfort. These birds may need toys, perches and cage accessories that cannot be chewed and ingested and may benefit from high fiber vegetables to fill this need.
With patience, perseverance, prolonged therapy, and attention to correction of secondary problems, many birds affected with PDD can be returned to health. Life expectancy at this time cannot be predicted.
References
1. Kistler AL, Gancz A, Clubb SL, et al. Recovery of divergent avian bornaviruses from cases of proventricular dilatation disease: Identification of a candidate etiologic agent. Virology Journal, The electronic version of this article is the complete one and can be found online at: http://www.virologyj.com/content/5/1/88
2. Gregory CR, Ritchie BR, Latimer KS, et al. Progress in understanding proventricular dilatation disease, Proc Assoc Avian Vet, 200, pp. 269-276.
3. Dalhausen B, Aldred S, Colaizzi E. Resolution of clinical proventricular dilation disease by cyclooxygenase 2 inhibition, Proc Annu Conf. Assoc Avian Vet., 2002: 9-12.
SPEAKER INFORMATION
Susan L. Clubb, DVM
Rainforest Clinic for Birds & Exotics Loxahatchee, FL, United States 2009